Scope Definition (group scope)
Our project's scope pertains to an improvement in quality of life, a quite nebulous term that we have sought to more narrowly focus through the exploration of 3 very unique concepts:
- Accessibility needs among the elderly
- Engineering serendipitous community interactions
- Leveraging personal informatics and ubiquitous computing devices to facilitate more productive and actionable conversations between patient and practitioner
Ideation Process
Rather than ideate on one specific problem or provide alternatives to the same solution, the group instead created a whiteboard map of different problems, populations, augmentation methods and ideas as a method for both brainstorming and focusing ideas on specific problems. The group drew lines across dimensions (e.g., quality of life -> elderly populations in assistant home living -> technology accessibility) and then brainstormed possible ideas. The group then used dot voting to surface which of those ideas were most integral to the problems and populations and once three very solid ideas were decided upon, each group member explored those ideas in greater detail through observation, research and sketching. These more fully formed problems and ideas and expressed below.
As the iteration process continues, the group will move forward with one of these concept proposals based on feedback from faculty and peers.
As the iteration process continues, the group will move forward with one of these concept proposals based on feedback from faculty and peers.
Concept Proposals
1. Card-based Tangible Interface for Daily Tasks
Context and population
Elderly People (Although this can also be extended to people with visual impairments).
Motivations and observations
The motivation behind this concept comes from personal experience while interacting with elderly people. A majority of this set of audience is not very comfortable with using today’s technology. Their needs are not met in varying aspects of current technology innovations. They are generally used to physical buttons and tangible interactions and they have a limited set of tasks which they wish to accomplish during the day. But their ability to use modern day GUIs is primarily hampered by conflicting mental models, convoluted GUIs and physical disabilities like vision impairments, shakiness and so on.
Observations:
Observations:
- Elderly folk have a low tolerance for multiple sequence interactions and hence avoid using technology unless there is a compelling reason behind it.
- They are more used to tangible interactions (“push-button” like interfaces) and find them easy to use.
- Senior citizens find it difficult to map their mental models with today’s technology. For example, listening to music would involve finding the record/CD and placing it on the turntable/optical disk drive and pressing a button to start playing it. They can not map the same actions to today’s devices like apps and music-on-cloud.
- Visual impairments and other physical disabilities often hamper their ability to efficiently use touch screen interfaces.
- They are easily confused by the huge array of functions which modern day gadgets provide. Simplicity is key.
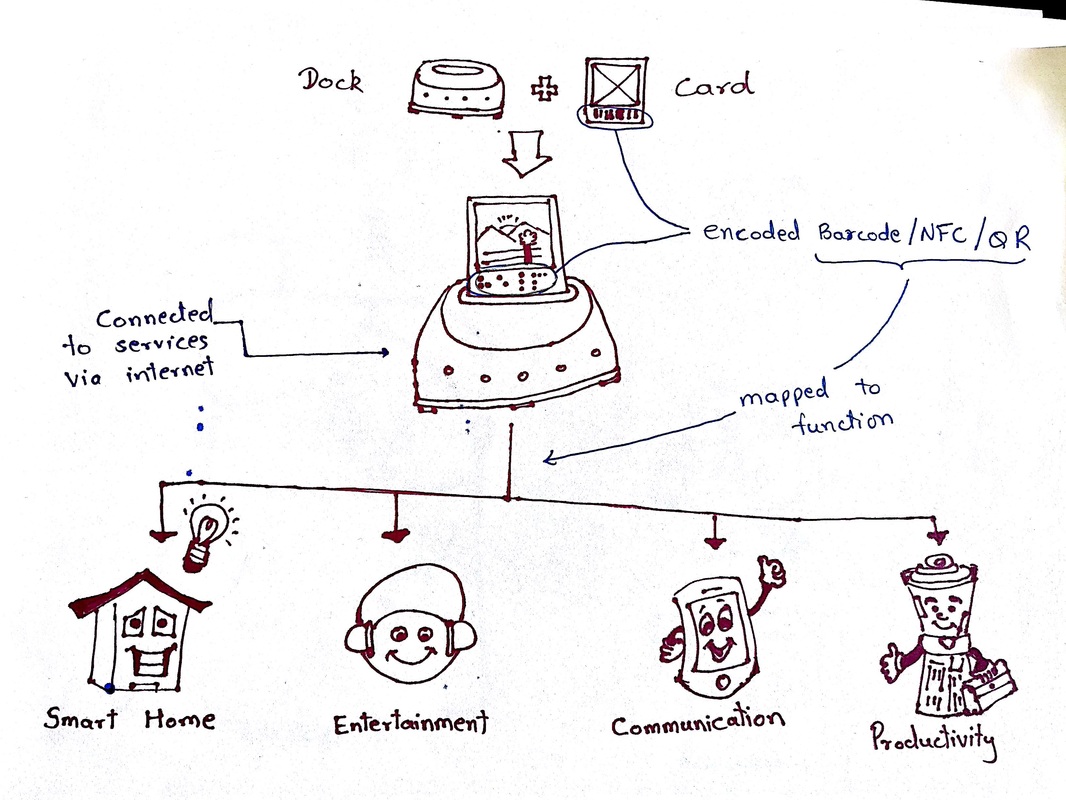
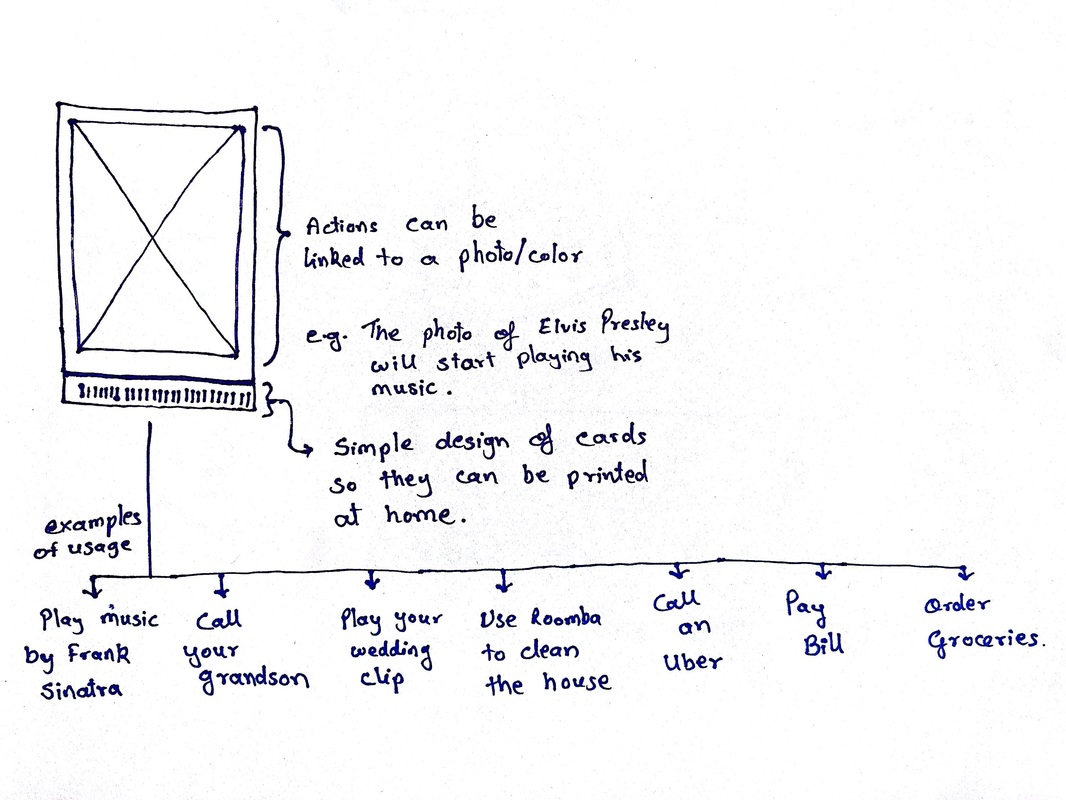
Concept
A physical card based modular interface which will help elderly people to make use of modern day technologies in a easy-to-use manner. The users will use paper cards which they can insert into a dock which will perform various actions using cloud and IoT technologies to provide services corresponding to the inserted card. These cards will be inexpensive and can be printed at home. The actions corresponding to them can be customized as per the user's’ preferences including the picture on the card or the color of it. This can be correlated to as a physical/tangible implementation of the IFTTT service. For example, if a user needs to start a video call to his/her grandson, inserting a card with a photo of him in the dock will initiate a video call to him/her. Another use could be playing audio/video on the television connected with the dock. The user could simply plug in a photo of his/her marriage and the video for it begins playing on the screen. This can be modularized using any service which provides an API for its service. This can range from media & entertainment, e-commerce, controlling your smart home and so on. The use of this product is not only limited to elderly people but users with visual or cognitive impairments. The appropriate needs for the users will need to be further researched to understand the requirement of such a product or service.
2. Community Interaction in public spaces
Context and population
The population for this design is the general public. There may be a reflex within HCI to focus on a more narrowly-scoped set of users, but making that an automatic stipulation would mean that public space is effectively beyond our concern as designers. So although this population is intentionally broad, there is a clear context of use: informal and playful interaction among strangers in public or semi-public spaces (e.g. malls, city squares, museum lobbies, parks, university campuses, and so on).
Motivations and observations
Due in part to the rise of personal ICT use (and partly due to the increasing privatization of urban space), it is becoming less and less common for strangers to have informal interactions with one another in publicly accessible places. So many people being ‘alone in public’ is hurting the quality of life in cities like Ann Arbor. I would like to see more thoughtfully designed spaces that facilitate spontaneous exchanges and make urban space feel more ‘alive’.
Even in places where informal interactions traditionally happen -- in cafes or on public transportation, for instance -- there is relatively little interpersonal exchange taking place. I observed customers waiting for their coffee to be prepared on four occasions in Starbucks, and observed that the vast majority of customers engaged with their phones to pass the time and did not speak to the other people waiting near them. Those who did engage in conversation either arrived together and already knew each other, or else recognized each other from a common class or previously shared activity. This avoidance of interaction may have been due to the discomfort that many people experience when conversing with strangers. What if strangers could communicate interactively in a more natural, nonverbal way?
Even in places where informal interactions traditionally happen -- in cafes or on public transportation, for instance -- there is relatively little interpersonal exchange taking place. I observed customers waiting for their coffee to be prepared on four occasions in Starbucks, and observed that the vast majority of customers engaged with their phones to pass the time and did not speak to the other people waiting near them. Those who did engage in conversation either arrived together and already knew each other, or else recognized each other from a common class or previously shared activity. This avoidance of interaction may have been due to the discomfort that many people experience when conversing with strangers. What if strangers could communicate interactively in a more natural, nonverbal way?
Concept
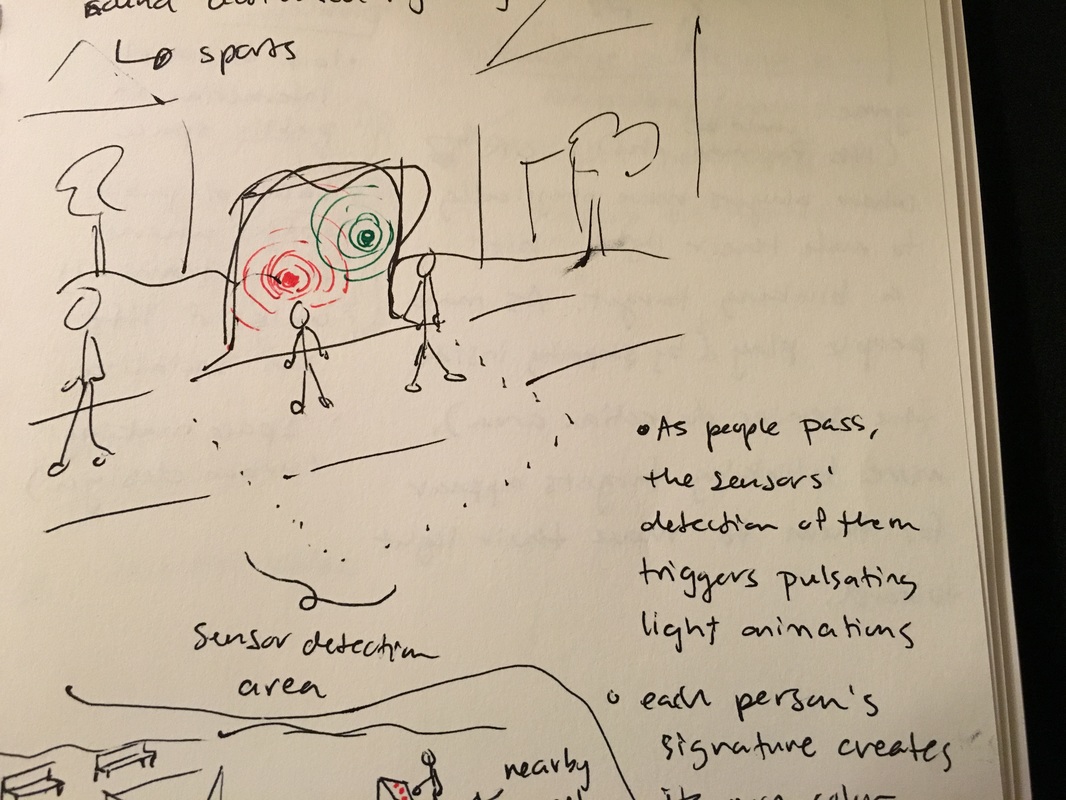
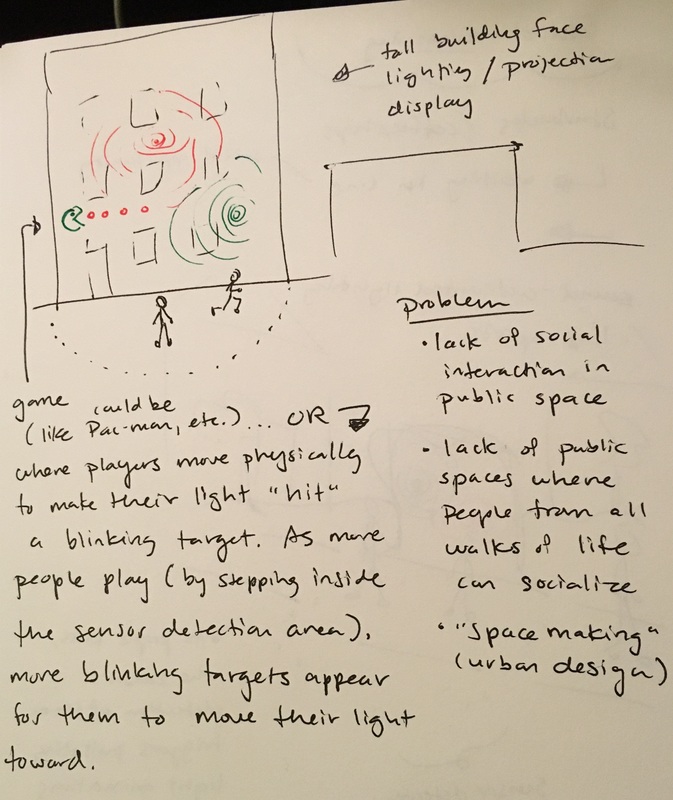
Interactive, playful lighting displays to spur informal interactions between strangers and create focal points that help enliven public or semi-public spaces. These displays would transform data generated by the motion of passers-by into fluctuations and animations in a visibly prominent LED-lit display. These installments could help increase the frequency and diversity of social interactions among strangers by helping them first communicate in a nonverbal, embodied way.
|
|
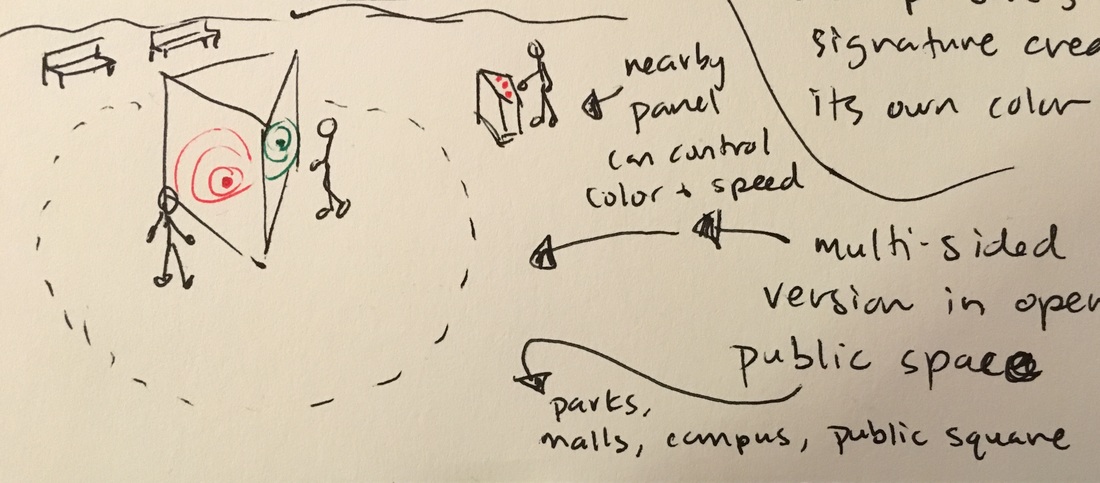
Sketch 2: This design includes a way for spontaneous creative collaboration between different participants. The people standing near the installment can control the directional movement of the lighting animation through their own movement and gestures. Meanwhile, from a nearby panel, others can alter aspects of the animation like color and speed of light fluctuation. This panel would create a secondary point of interaction in its own right, in addition to opening an opportunity for ‘movers’ and ‘controllers’ to communicate and coordinate with each other.
|
Sketch 3: This shows the light display on the face of a building. I started to image a Pac-Man-esque game that could be played, where users move within the space where sensors are to make ‘their’ color blobs ‘chase’ and ‘catch’ another light blob. This kind of installation might be more practicable if done with some sort of light projection rather than placing lights on the side of an entire building.
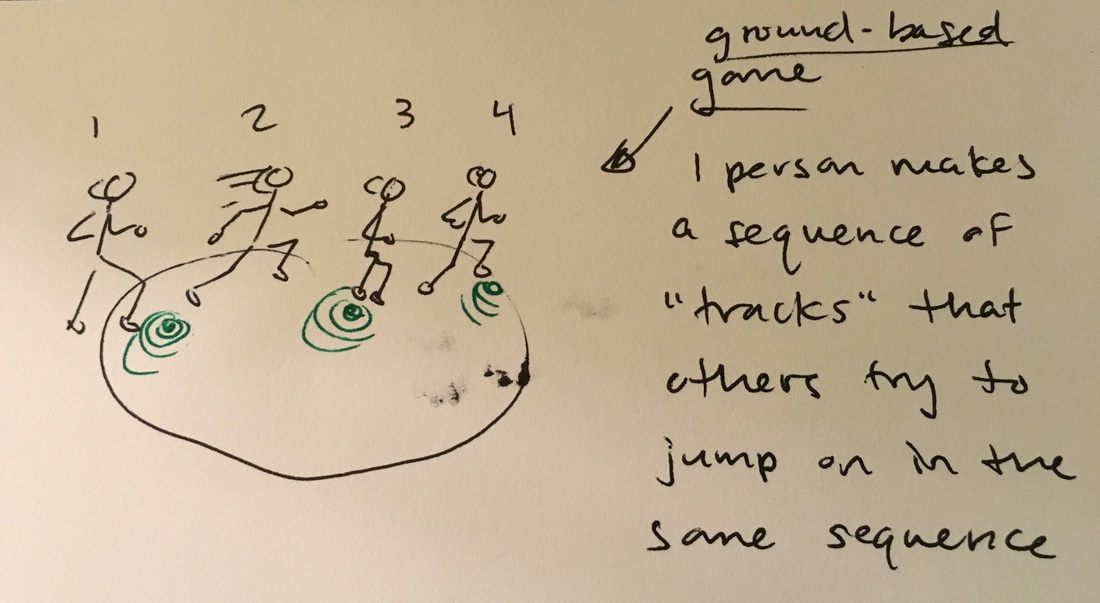
Sketch 4: In this idea, the lights are placed on the ground.
|
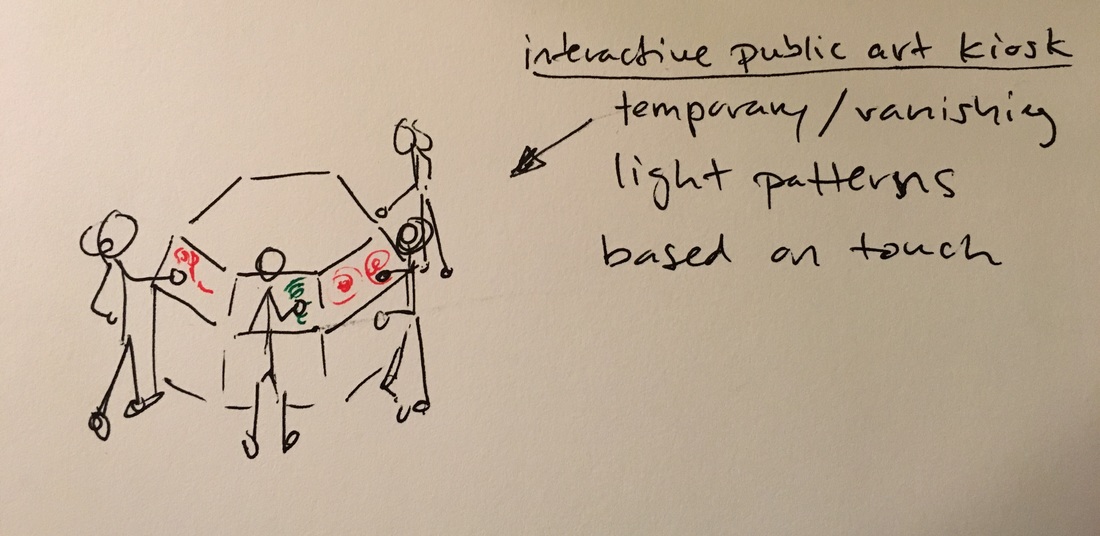
Sketch 5: This shows a display where motion or touch create temporary strokes of color (visible in a light-based display or potentially a digital screen). The different ‘canvases’ are joined together in a way that makes each person’s composition partly within the view of the person next to them -- creating a natural bridge to conversation and shared experience. This idea is partly drawn from the image of a sand drawing; the strokes would not remain longer than a few seconds. This would discourage people from monopolizing the interfaces, because they would need to constantly create new drawings in order to ‘use’ the space continuously.
|
3. Mood Watch
Context and population
According to the University of Michigan’s MI Talk Website, “42.1% [of students] said they had felt so depressed that it was difficult to function at least once during the school year” whereas about 6.7% of the American population aged 18 and older are affected by major depressive disorder. Given how dramatically higher the depression rate is among University of Michigan students compared to the overall American population, a ubiquitous interaction design is worth exploring in order to hopefully alleviate mental health issues facing an estimated 18000 students. The University of Michigan could be a test-bed for such an area of research and depending on results, scalable to other universities, hospitals and assistant care living centers.
Further compounding this problem is a lack of productive patient-practitioner interactions. Systems like M-DOCC do exist, which sends monthly emails to enrolled members that serve as “check-ins” in the form of questionnaires a user fills out. In the event that questionnaire results reveal spikes in anxiety or depression, M-DOCC will call that patient and work to set up an appointment with their primary care provider; however, these questionnaires suffer from recency and satisfying biases that could mask true capture of depressive symptoms and limit a caregivers ability to more thoroughly target the underlying causes. Thus, having management or tracking tool that is accessible by the patient at all times and track on a more continual and ongoing format could provide richer data to the practitioner vs. what is currently available. Products do exist, such as the Mood Watch App and AffectAuro, but these are decoupled from the patient-practitioner relationship and could potentially result in inaccurate self-diagnosis or hypochondriac behavior among their users.
References:
1 https://mitalk.umich.edu/suicide
2 http://www.ro.umich.edu/report/15enrollmentsummary.pdf
3 http://www.dbsalliance.org/site/PageServer?pagename=education_statistics_depression
4 http://www.depressioncenter.org/
5 https://www.uhs.umich.edu/depression
6 https://mitalk.umich.edu/mentalhealth
7 https://caps.umich.edu/
8 http://www.pewresearch.org/fact-tank/2015/08/20/how-having-smartphones-or-not-shapes-the-way-teens-communicate/
9 http://affect.media.mit.edu/pdfs/12.McDuff-etal-AffectAura.pdf
10 http://www.moodwatchapp.com/
Further compounding this problem is a lack of productive patient-practitioner interactions. Systems like M-DOCC do exist, which sends monthly emails to enrolled members that serve as “check-ins” in the form of questionnaires a user fills out. In the event that questionnaire results reveal spikes in anxiety or depression, M-DOCC will call that patient and work to set up an appointment with their primary care provider; however, these questionnaires suffer from recency and satisfying biases that could mask true capture of depressive symptoms and limit a caregivers ability to more thoroughly target the underlying causes. Thus, having management or tracking tool that is accessible by the patient at all times and track on a more continual and ongoing format could provide richer data to the practitioner vs. what is currently available. Products do exist, such as the Mood Watch App and AffectAuro, but these are decoupled from the patient-practitioner relationship and could potentially result in inaccurate self-diagnosis or hypochondriac behavior among their users.
References:
1 https://mitalk.umich.edu/suicide
2 http://www.ro.umich.edu/report/15enrollmentsummary.pdf
3 http://www.dbsalliance.org/site/PageServer?pagename=education_statistics_depression
4 http://www.depressioncenter.org/
5 https://www.uhs.umich.edu/depression
6 https://mitalk.umich.edu/mentalhealth
7 https://caps.umich.edu/
8 http://www.pewresearch.org/fact-tank/2015/08/20/how-having-smartphones-or-not-shapes-the-way-teens-communicate/
9 http://affect.media.mit.edu/pdfs/12.McDuff-etal-AffectAura.pdf
10 http://www.moodwatchapp.com/
Motivations and observations
Due to the proliferation of mental health issues on the University of Michigan campus and observation of the process that the University of Michigan Health System provides, two distinct, but connected, user groups (patients and practitioners) have similar motivations. They want to alleviate depressive symptoms, engage in more enriching and targeting dialog about the patient's feelings and mood changes and investigate the sources of depression and anxiety so that more personalized treatment plans can be created. This all has to be done quickly and succinctly as patients may not have the financial flexibility for multiple sessions nor do health agencies have the staffing necessary to provide each patient with as much care and attention as the practitioner feels they deserve.
Because of HIPAA ethical compliance, observing these interactions directly is impossible. Instead, observations were centered around the M-Strides program as noted above. The process goes as follows:
Some of the things noted from this observation are:
Because of HIPAA ethical compliance, observing these interactions directly is impossible. Instead, observations were centered around the M-Strides program as noted above. The process goes as follows:
- Patient receives monthly automated email asking them to complete questionnaires
- P opens attachment that links to the secure email
- P opens the secure email
- P logs onto M-Strides
- P is presented with 3 questionnaires to complete (GAD, MDOCCADDL and PHQ)
- P completes GAD (general anxiety disorder) questionnaire
- P sees a histogram of their anxiety scores over the last several months
- P completes MDOCCCADDL questionnaire
- P completes PHQ (patient health questionnaire) which focuses on depressive symptoms
- P sees a histogram of their depression scores over the last several months
- System confirms that everything is complete
- If scores are alarming, patient receives a call from an individual within M-Strides urging them to contact their health care professional
Some of the things noted from this observation are:
- Scores provided lack context and explanation by a trained professional
- The system relies on 12 steps in order to facilitate an interaction
- The patient provides information at a time when they are likely less burdened by depressive symptoms
- These questionnaires are not capturing "in-the-moment" data about a patient's mental health state
- They are not used to open a dialogue about when and where a patient was feeling depressed or anxious, rather these questionnaires just serve as a multi-step process for urging a patient to contact their health care provider
- The phone call may be too intimidating for a patient that does not already have a relationship or rapport with a specific practitioner or therapist and thus may continue going untreated
Concept
With those observations in mind, the below proposal may help ameliorate some of the issues noted. A patient could be prescribed a wearable by their health care practitioner, allowing them to track mood changes in real time. This watch could potentially also collect other information either passively, such as time or GPS (though this may depend on the user's comfort) or when the user turns the watch to indicate a mood change the watch may prompt the user to provide some additional information, building out better context and map their mood to whatever is happening in that moment.
The data is stored on the watch and then downloaded onto the practitioner's computer where they review it with their patient. This ensures that there is proper context and diagnosis and ultimate serves to facilitate more meaningful conversations that could potentially result in better treatment plans. Though this technology already exists, the emphasis here is on a simpler technology that is embedded in the patient-practitioner relationship rather than a novelty item that is ultimately left up to the user to interpret or potentially misinterpret.
The data is stored on the watch and then downloaded onto the practitioner's computer where they review it with their patient. This ensures that there is proper context and diagnosis and ultimate serves to facilitate more meaningful conversations that could potentially result in better treatment plans. Though this technology already exists, the emphasis here is on a simpler technology that is embedded in the patient-practitioner relationship rather than a novelty item that is ultimately left up to the user to interpret or potentially misinterpret.
|
|
|
